Access to early diagnosis remains uneven—but that is beginning to change. Advances in portable, AI-enabled diagnostics are bringing faster detection closer to last-mile communities, enabling earlier intervention and more resilient health systems. https://t.co/j78SQZAd8F
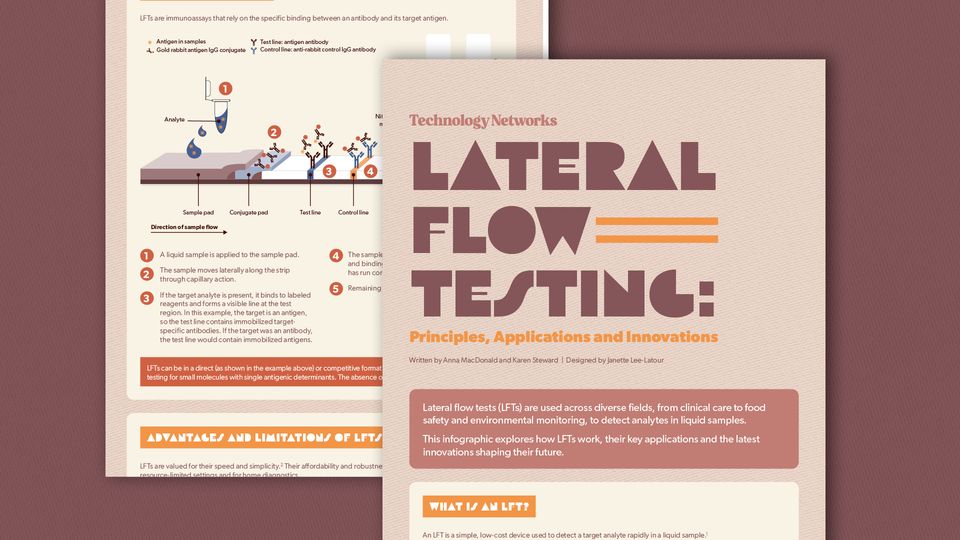
An infographic describing lateral flow (point-of-care) tests: how they work, key applications, advantages/limitations, and recent innovations (including smartphone/reader integration and AI image‑analysis). It directly supports the tweet by showing a high-quality visualization of portable diagnostics used at the last mile and how digital/AI-enabled readers are improving early detection and data sharing in low-resource settings.
Source: Technology Networks
Research Brief
What our analysis found
Access to early diagnosis in underserved communities remains one of healthcare's most persistent challenges. In the United States alone, nearly 92% of rural counties lack sufficient primary care physicians, with some counties having no primary doctor at all. Rural areas average just one physician for every 2,881 residents, and over the past decade, more than 100 rural hospitals have closed, with at least 600 more—roughly 30% of all rural hospitals—at risk of shutting down due to funding shortfalls. These gaps translate directly into higher mortality rates for rural populations, who often face long travel distances and delayed care.
However, a new wave of portable, AI-enabled diagnostic tools is beginning to reshape this landscape. The federal government's PARADIGM program, launched in 2025 through the Advanced Research Projects Agency for Health (ARPA-H), is funding scalable mobile platforms designed to deliver advanced medical services outside traditional hospital settings. Mission Mobile Medical Group was awarded up to $26 million to develop next-generation mobile clinics, while the University of Michigan received up to $25 million to build an AI agent called VIGIL that enables general practitioners to perform specialist-level diagnostics. Meanwhile, ultraportable imaging devices, AI-powered cough analysis achieving 86% accuracy in TB screening, and cataract screening tools with 81.2% sensitivity and 94.3% specificity are demonstrating real clinical value in resource-scarce settings.
The economic case is also compelling. According to Accenture, AI implementation could generate savings of up to $150 billion for the U.S. healthcare system by 2026. Yet significant hurdles remain, including the digital divide in rural areas, algorithmic bias risks, regulatory uncertainty, and high upfront costs—all of which temper the optimism surrounding these technological advances.
Fact Check
Evidence from both sides
Supporting Evidence
ARPA-H PARADIGM Program funding real-world deployments
The federally funded PARADIGM initiative, launched in 2025, is actively developing scalable mobile medical platforms. Mission Mobile Medical Group received up to $26 million for next-generation mobile clinics with initial deployments expected by mid-2025, and the University of Michigan received up to $25 million to build the VIGIL AI agent for mobile diagnostic support.
AI-guided diagnostics proven effective in rural and resource-limited settings
Studies have demonstrated that AI-powered tools can achieve 86% accuracy in tuberculosis screening through cough analysis and 81.2% sensitivity with 94.3% specificity in cataract screening deployed in rural communities, supporting the claim that faster detection is reaching last-mile populations.
Ultraportable medical imaging reduces dependency on specialists
Handheld ultrasound devices and mobile X-ray units equipped with AI guidance allow non-specialists to perform and interpret diagnostic imaging in settings that lack radiologists or traditional laboratory equipment, directly extending diagnostic capacity to underserved areas.
University of Florida's Multi-Tags AI system empowers nonspecialists
As part of the PARADIGM program, UF is developing an AI system designed to guide family members, social workers, and community health staff through basic medical tests including blood draws and diagnostics, effectively bringing hospital-level care to remote communities.
Significant projected cost savings bolster sustainability
Accenture estimates that AI implementation could save the U.S. healthcare system up to $150 billion by 2026, suggesting that AI-enabled diagnostics could be economically viable at scale and contribute to more resilient health systems.
Contradicting Evidence
The digital divide poses a fundamental barrier to deployment
Rural areas frequently lack reliable internet connections, sufficient computing infrastructure, and technical expertise needed to operate AI-enabled diagnostic platforms, which could severely limit the scalability and effectiveness of these technologies in the very communities they aim to serve.
Algorithmic bias risks worsening existing health disparities
AI diagnostic algorithms trained predominantly on data from urban, well-resourced populations may produce inaccurate results when applied to rural or underrepresented groups, potentially leading to misdiagnoses and deepening the health inequities the technology is meant to address.
Regulatory hurdles slow the pace of real-world adoption
AI-based medical technologies must undergo rigorous FDA safety and effectiveness assessments, a process that can be slow and uncertain. Regulatory ambiguity around decision ownership when AI is used in triage or diagnostics also creates potential liability concerns that may delay deployment.
High upfront costs and ongoing maintenance challenge sustainability
While portable AI solutions may prove cost-effective over time, the initial investment in technology acquisition, integration into existing workflows, continuous monitoring, and governance infrastructure can be prohibitive for resource-constrained rural health systems.
Concerns about dehumanization of care persist
The increased reliance on AI-driven diagnostics raises ethical questions about reduced patient-provider interactions and the potential dehumanization of healthcare delivery, particularly in communities where trust and personal relationships with providers are central to health-seeking behavior.
Report an Issue
Found something wrong with this article? Let us know and we'll look into it.